As an executive at Google, Eve McDavid had a lot of energy and wherewithal to devote to complicated problems. And so, after her cervical cancer treatment, she knew exactly where she would place her skills: developing a better device for treating other women with cervical cancer. The famously entrenched problem was not too daunting or too big for her: “I come from technology. I’m an executive,” she says. “I have a 30,000-foot view.”
She then founded Mission-Driven Tech, where she’s also the CEO, to help improve brachytherapy, an essential intervention for almost all later-stage cervical cancers. Brachytherapy hasn’t meaningfully changed in fifty years— and this dangerous lag in updates means that hundreds of thousands of women are dying unnecessarily, and encountering potentially avoidable side effects. The field remains underfunded, fragmented, and burdened by stigma.
In Eve’s conversation with Jadey, she speaks about the gaps between prevention, screening, technology and treatment— as well as how her experience changed her relationship to motherhood, self-expression, and communication.
Q:
If there were one myth about cervical cancer you could dispel once and for all, what would it be?
A:
The myth I would dispel is that cervical cancer is rare or only affects a small number of people. Cervical cancer is not uncommon, and it is not rare. HPV, the virus that causes it, is involved in at least 350,000 global deaths each year and in at least 5% of all cancer diagnoses affecting men and women. That includes cancers of the cervix, anus, rectum, vagina, vulva, and head and neck, with instances of prostate and colorectal cancers also influenced by HPV.
Cervical cancer’s root cause, HPV, is contracted by nearly every unvaccinated person on the planet through sexual activity at some point in their lifetime. About 120% of those infections are oncogenic strains, meaning they can lead to cancer. So when this disease is described as rare, we fundamentally know that is not true. It is a common disease, and it is not rare.
Q:
You’ve spoken about cervical cancer at the White House Cancer Moonshot and been recognized by the World Health Organization. What narratives are missing that you’re determined to bring to light?
A:
Number one is: What happens if we don’t catch a woman in prevention and screening? What does her diagnosis and treatment mean for her? And number two: Where is the funding in this field, and why hasn’t it arrived yet?
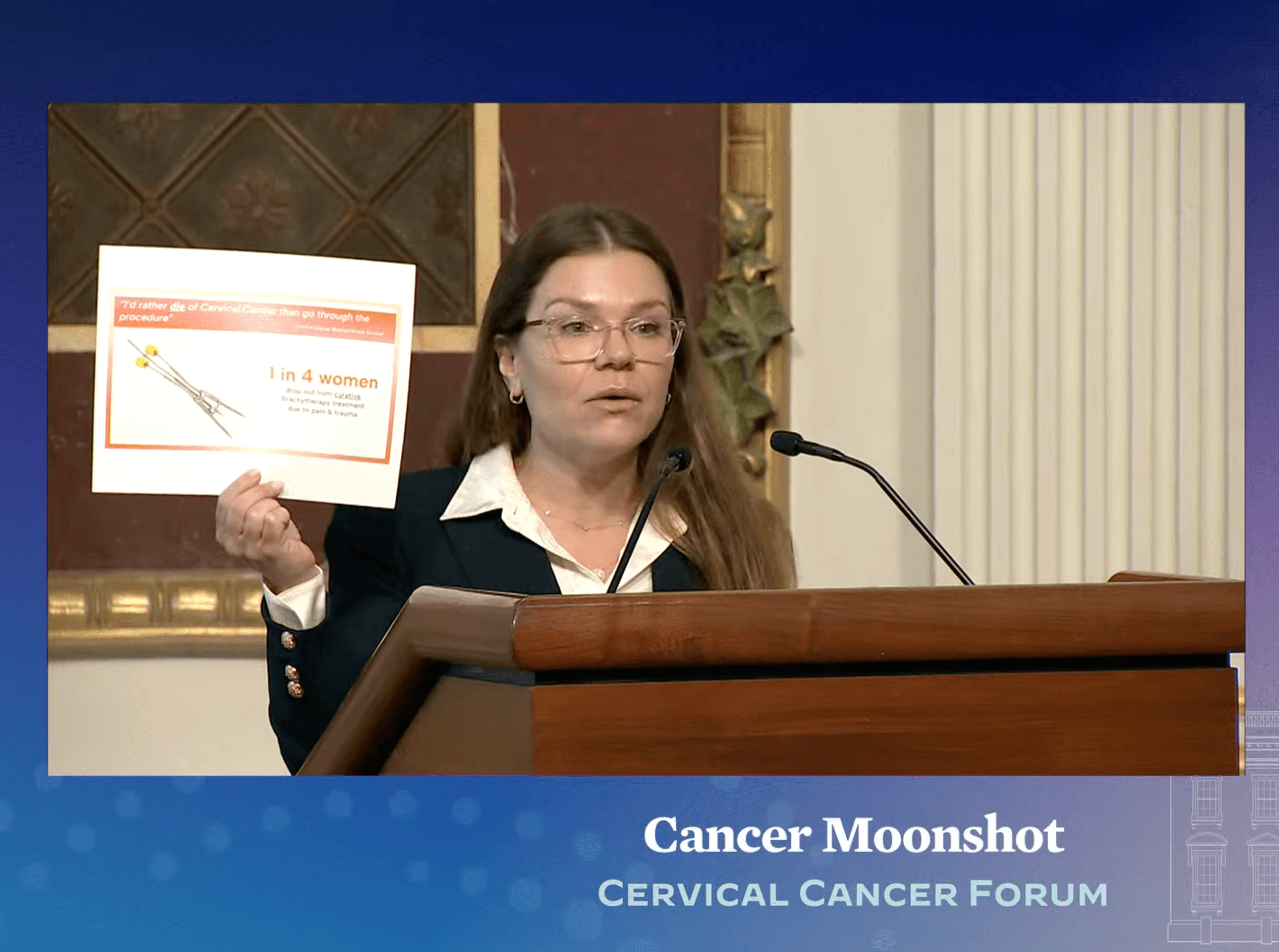
Eve McDavid speaking about cervical cancer at the White House.
Q:
Why do you think funding or research has been attentive enough to this? Why isn’t this treated more seriously?
A:
I was just at the JP Morgan healthcare conference in San Francisco with CEOs, investors, oncology leaders, medical device builders, and women’s health executives. Every leader in the building said: the female body was not studied. Women were not included in clinical trials until 1993 and equitable inclusion has really only happened in the last 10 to 15 years.
When you have an under-researched area that affects 51% of the population, and you don’t have specific research around how health events are experienced in a female body, you don’t have scientific data. You don’t have clear communication to the marketplace about what problems exist and what solutions address them. And without defined scientific research in healthcare, you cannot get to market. You cannot bring new solutions, new therapies, new treatments. It’s highly regulated. The research is a reflection of the investment. Nothing happens for free. If you’re not in the research, nothing is happening.

Eve McDavid speaking about cervical cancer at Cornell Tech.
Q:
Something you’re vocal about is the particular stigma of cervical cancer impacting the lack of investment in the cure. Can you tell us more about your perspective there?
A:
In [cervical cancer], there are gaps in field funding and gaps in field leadership. First, it’s caused by a sexually transmitted infection and, culturally, we do not have a comfortable dialogue around sexual health, infection, and illness.
When I was diagnosed in 2020, I told people only that I had cancer. I did not say cervical cancer, I did not say HPV. I did not say cervix. When you’re told you may not have many mornings ahead, and the diagnosis is tied to sexual activity, infection, infertility, menopause, death: you shrink. I thought: the only person I can tell is my husband. I would whisper to him that I’m really concerned.
Second, despite under-prioritization, there is an established cure. Brachytherapy, the area I focus on [at Mission-Driven Tech], has been curing people for decades. But the process has high treatment toxicity and is so painful that many women do not complete it. Practitioners are using medical devices that haven’t been updated in fifty years.
The HPV vaccine was first released in 2006. In some countries like Australia and in the U.K., they administer [the vaccine] in public middle schools; and they have no incidence of cervix cancer in those populations 20 years later. In the past 50 years of Pap testing, we’ve seen cervical cancer rates decrease by half.
We have the building blocks moving in the right direction. But we don’t have a clear through line across the care continuum. That’s my 30,000-foot view. I come from technology. I’m an executive. This is what I can and should move.

Eve McDavid speaking about cervical cancer for NY State Innovation.
Q:
Tell us more about Mission-Driven Tech and how it could be an intervention into this care.
A:
Mission-Driven Tech is a cervix cancer innovation company. We are building solutions to address the problems that exist in cervical cancer today.
Our core product in development is a modern brachytherapy medical device. Brachytherapy is internal radiation: a catheter system that brings a high-dose boost of radiation directly to the tumor so you can melt the tumor, disrupt the HPV virus, and spare healthy surrounding tissue and organs. It dates back to Marie Curie’s discovery of radium. It is the most effective component of standard of care. You cannot survive a Stage 1B or later diagnosis, which represents about 70% to 80% of global diagnoses, without brachytherapy.
But the devices we use today were designed in the 1970s. The procedures can last eight to ten hours, often with very little anesthesia. Women may be cured, but their outcomes are poor because the surrounding healthy tissue [can be impacted]. The experience is so jarring and traumatizing. The placement and then the removal of the device is excruciatingly painful. You're immobilized while awake with the device inserted for hours. This experience is so terrible, that up to 40% of women drop out before completing treatment, knowing that if they drop out, their tumor may recur and they can die. They are actively choosing dying over completing the cure.
As a survivor of these procedures and a student of systems and technology, I know those two facts don’t belong together: there is a cure and it is too difficult to complete. So the goal is to take the cure from something that works, but is brutalizing, to something that works and isn’t brutalizing.
Q:
Can you tell us more about what it’s like to develop a medical device?
A:
Medical device development is highly regulated. The science must be reviewed by the government—the NIH, the FDA, CMS. It requires enormous capital, time, and expertise. And as a female founder in a category where only 2% of venture capital dollars go to ventures like ours, the hurdles are extraordinary.
So we do two things at once: we follow the defined regulatory path for our north star device, and we build solutions we can ship now. Our R&D has generated additional products and initiatives that address gaps across the care continuum—from education to informed consent to procedure safety.
For example, a UK study shows that half of women cannot identify their cervix on a diagram. So we created a happy, healthy cervix logo to normalize what this organ is and what it looks like. We created physical products to put a cervix on the desks of decision-makers.
We produced research called “BrachyStories,” featuring international survivors of brachytherapy. At the 2024 World Congress of Brachytherapy, it was the first time gynecologic survivors’ videos were shown publicly (while prostate patients are routinely invited to speak). Doctors practicing for years said: I can improve informed consent language tomorrow. I can improve pain management tomorrow.
And so by presenting it in this way to these audiences, building with clinicians, we are making this an invitation for innovation. We’re positioning ourselves as a credible partner and problem solver. If we hit our roadmap, we hope to share data with regulatory bodies before the end of next year.

Q:
What should women understand about pregnancy and cervical cancer? Or even what we don’t understand yet about it?
A:
Since my diagnosis, I’ve met many women diagnosed during or around pregnancy. Pregnancy may be a risk factor if you enter it with an established high-risk HPV infection. Biologically, the immune system adapts during pregnancy to recognize the fetus as its own, peeling back defenses. If there’s a dormant infection, those changes can allow the virus to strengthen and replicate. Add the extraordinary blood flow to the pelvis and changing anatomy, and it can be an explosive combination.
On the lived side, there are unlimited ways to feel like an insufficient mother with this diagnosis. Some women lose the chance to have children. It strips mothers and families during our breadwinning and childbearing years.
Q:
Can you tell us a little more about parenting through this?
A:
I had two healthy children. I entered motherhood part two [after diagnosis] underprepared, with a newborn, a toddler, and a life-threatening diagnosis. In the aftermath, as my children were potty training, I was relearning bladder and bowel function. There are striking parallels.
And yet, because of the healing work, I am a more present mother. Instead of being on planes half the month, I work from my home office, drop my kids at the bus, pick them up. When I travel, it’s to accelerate the cure for cancer. My children know my work is to help the sick queens, because all the sick queens need help too. So this has enabled me to be a more whole mother, a more compassionate, empathetic and patient mother. And frankly, it’s given me the humility that I needed with my children.
Q:
How do you talk to your children about all of this?
A:
My kids have grown up knowing what a cervix is, that viruses can cause cancer. I was in menopause at 33 and taking hormone replacement therapy. Without it, quality of life after treatment is extraordinarily difficult. On vacation once, I forgot my prescription and panicked. I told my kids, if mama doesn’t have her medicine, she’ll be like Strega Nona inside after treatment: like a woman who went 40 years ahead on her timeline. There are ways to bring a family through this that integrate reality without fear.